The great French physiologist Claude Bernard developed the concept of the milieu intérieur: the delicately regulated fluid environment that surrounds our cells, courses through our arteries and veins, bathes every muscle and nerve, organ and bone in our bodies. Kidneys do many things to maintain the equilibrium, or “homeostasis,” of this fluid environment. They remove substances of varying molecular sizes from our blood, which our body produces as it makes and burns energy—by-products that become toxic if they accumulate. (The liver removes other chemicals directly after digestion, including alcohol and drugs, while the bowels, lungs and skin perform additional excretory functions.) While sieving these toxins from our bloodstream and voiding them as urine, the kidneys also conserve scores of essential blood components, preventing their loss during urination. And kidneys manufacture a number of hormones and vitamins that control bodily processes like red blood cell production, blood pressure regulation and bone building.
Kidneys even have a sense of smell. To sift hundreds of blood and urine chemicals on the fly, expelling some and husbanding others in precise quantities, kidneys employ odor receptors similar to those found in the nose. “The kidney is sniffing the urine and the blood plasma as they go by,” says Jennifer Pluznick, associate professor of physiology at the Johns Hopkins School of Medicine, who discovered the organ’s olfactory gifts. “The kidney’s attention to detail is astounding. I’m convinced it has many other long-held secrets which are waiting to be discovered.”
For the first time, doctors had managed to substitute a machine for a vital organ.
Even for people who spend their whole lives studying them, kidneys are mysterious.
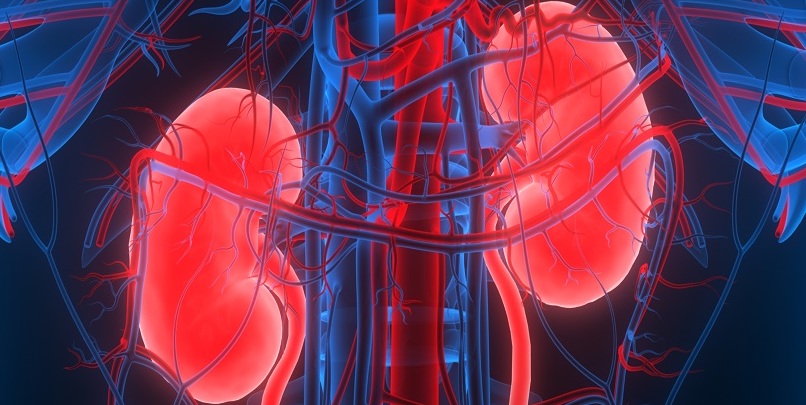
The heart tells with every beat how vital the kidneys are. Twenty percent of the blood of every pulsation goes straight to the kidneys, which receive four times more blood by weight than the liver, seven times more than the brain, and fourteen times more than the lungs. A healthy pair of kidneys cleans one liter of blood per minute, which means that every five minutes they purify the entire blood volume of a 150-pound adult. As blood traverses the kidneys, the components it holds in solution dance back and forth across various membranes and gradients, in an intricate quadrille of filtration and reabsorption that ultimately produces two separate streams: hyperclean blood and fragrant urine. The blood resumes its restless rounds throughout the body, while the urine travels down the ureter into the bladder, and out through the urethra into the open air.
Blood pumps from the heart to the kidneys down the renal arteries, and diffuses throughout a series of microscopic tubular structures called nephrons, the kidney’s functional unit; a healthy young kidney contains about a million nephrons. Each nephron is a filtration system consisting of a tuft of capillaries called the glomerulus, which drains into a long, convoluted tubule. The glomerulus performs “ultrafiltration”: high-pressure arterial blood straight from the heart hits the cell walls of the glomerulus, a multilayered membrane with pores about four nanometers across. Larger blood components like red and white cells and the bigger plasma proteins are held back by the glomerular wall, while smaller molecules of waste, and much of the water they’re dissolved in, press through the pores into the nephron tubule beyond.
The liquid that collects on the far side of the glomerular wall, the “ultrafiltrate,” is the first phase of urine production, and henceforth travels through the kidneys independently from the blood. But this liquid, which resembles blood plasma without its proteins, still contains many substances that our organism has always craved—salt, glucose, amino acids, electrolytes and water, always and forever water. The glomeruli produce about 180 liters of ultrafiltrate a day; if we simply pissed this liquid away, we would dehydrate and die in minutes. To avoid this, the tubule into which each glomerulus drains, with its hairpin curves, ascending loops and other convolutions, recaptures these life ingredients and returns them to the blood. Of the original 180 liters of ultrafiltrate that our kidneys produce daily, we actually void only 1.5 to 2 liters of carefully concentrated, miraculously sterile urine, redolent of phosphates, urea and other wastes. And occasionally, of asparagus.
Kidneys fail for many reasons. Time itself wears them out: between our twenties and our seventies, most of us lose half of our renal function, through a gradual atrophy of the nephrons. Some people are born with hereditary conditions and developmental malformations that accelerate the natural renal decline. Inflammatory and autoimmune diseases can also damage our nephrons, as can a sudden injury, a heart attack, or any other mishap that cuts blood flow to the kidneys. Signs of these ailments have been found in the kidneys of Egyptian mummies, and among notables of later times. Mozart seems to have died of kidney failure after a severe strep infection, Buffalo Bill Cody lost his kidneys after prolonged use of headache powders (a similar analgesic, Bex Powders, caused a rash of kidney disease in post–World War II Australia), and George Bernard Shaw expired from acute kidney injury after falling from a fruit tree he was pruning. More recently, Veronica Lake’s kidneys packed up after an extended bout of cirrhosis, Dexter Gordon lost his kidneys to cancer, and chess prodigy Bobby Fischer died when a urinary tract blockage, for which he refused medicine or surgery, led to kidney failure.
In the past few decades, diabetes, obesity and hypertension have become health epidemics in the West, and are now the three main causes and accelerators of renal failure, because each condition damages or increases strain on the kidneys (in the United States, more than 60 percent of all patients newly diagnosed with renal failure also have diabetes). Certain medications also harm our nephrons, the worst offenders being nonsteroidal anti-inflammatory drugs like ibuprofen—the modern-day successor to Bex Powders—as well as some antibiotics, blood pressure medicines and chemotherapy drugs. Today, about 37 million adults in the United States are estimated to have some degree of renal disease, and nearly 800,000 have kidney failure. These numbers were still on the rise in 2020, when COVID-19 decimated the dialysis population. In 2020, for the first time since the US government began recording statistics on renal failure in 1973, the number of patients on dialysis dropped.
To confront the ancient curse of kidney failure, medical science devised dialysis. From the end of World War II through the 1960s, doctors in Europe and North America built a variety of instruments that could rid the patient’s blood of some of the wastes and excess fluid that healthy kidneys naturally remove. Teams of doctors and brilliant loners, many of whom were gifted engineers and tinkerers as well as healers, cobbled together blood-purifying gadgets from sewing machine motors, ice-cream makers, aircraft parts and sausage casings, and invented novel ways to connect them to the circulatory system of their patients.
In so doing, they made medical history. For the first time, doctors had managed to substitute a machine for a vital organ, halting the progression of a hitherto fatal illness, and sometimes postponing death for decades. A new branch of medicine was born, “nephrology,” from nephrós, Greek for “kidney.” Progress in dialysis went hand in hand with the evolution of kidney transplantation, and of allied therapies to suppress the immune system so that the recipient’s body would more readily accept the donor organ. In 1954, doctors at the Peter Bent Brigham Hospital in Boston, a teaching hospital for Harvard Medical School that is now part of Brigham and Women’s Hospital, performed the first successful transplant of a major internal organ, removing a healthy kidney from Ronald Herrick and grafting it into his identical twin brother, Richard, a victim of incurable kidney disease. Lung, liver, pancreas and heart transplants soon followed.
This was a heroic age of medicine, which saw revolutionary surgical procedures and novel devices gain ground on a host of once fatal conditions. It was a period of intense intellectual excitement, as polymath doctors armed with new technologies joined battle with some of humankind’s most intractable enemies, and seemed to be winning. It was an international age, where physicians in medical centers in Seattle and Boston, Toronto and Paris, but also in small town hospitals in Sweden and Holland, created hubs of advanced kidney expertise, to which other doctors traveled from around the world like pilgrims to a shrine, to return home after absorbing the new wisdom of nephrology, and become disciples in their own right.
If dialysis is stagnating worldwide, it is in crisis in the United States.
In New York, Leonard Stern, who founded the dialysis program at Columbia University, remembers his medical school training and residency in the early 1970s, in a fledgling specialization that had just received a name. “I took to nephrology immediately, because it fed into my need to know how things worked. It was the only specialization at that point where you could examine the metabolic condition of the patient, identify a disorder, and intervene in the hope of correcting it. If you went into gastroenterology back then, you had no idea how anything worked in the GI tract—it just happened. Or in dermatology, you had a thousand different conditions, yet no idea of the mechanism or the cause behind any of them. Whereas in nephrology, you could actually decide, ‘Well now, this is what most likely happened. So the patient feels this, and then we can dissect how they got there.’ For me, nephrology became a way of thinking about the world, and about the whole patient—not just the kidney.”
In the same years, on the far side of the world in Melbourne, John Agar, who was awarded the Order of Australia in 2009 for services to renal medicine, remembers how he and his peers saw nephrology as “a field of infinite promise.” After completing his nephrology training in Melbourne and spending an additional year at the University of Massachusetts Medical Center, Agar founded a dialysis unit at Geelong, southwest of Melbourne, whose methods and guiding philosophy helped to shape the practice of nephrology throughout Australia and New Zealand. He also spent a pivotal period of work at the University of Toronto, where he learned the latest techniques being used in home nocturnal dialysis, a groundbreaking treatment method.
“When I began my nephrology training in 1972, it was a thrilling field in rapid growth,” says Agar. “This seemed like the future of medicine. We were streets ahead of gastroenterology and cardiology. We were the only specialty that could replace a vital organ. Not only could we replace it artificially, but we could replace it with a new, transplanted organ. I was racing around Melbourne with an Esky cooler that contained donor kidneys! We were also on the cusp, or so we thought, of xenotransplantation: we were going to be able to transplant pig organs, monkey organs, even to breed special animals that would provide us with an infinite number and array of transplant kidneys, without need for a human donor at all. And dialysis was about empowering the patients: not only saving their lives, but giving them the skills to take charge of their own care. When I started nephrology, all this was happening.”
Since 1972, across the world, the original promise of dialysis has faded. The new technology used to treat individuals with kidney failure, which exhilarated young doctors like Leonard Stern and John Agar in the 1970s, has not evolved significantly in half a century. “What was infinite promise, is now infinite disappointment,” says John Agar today. But if dialysis is stagnating worldwide, it is in crisis in the United States, where the incidence of infection, heart problems and other dialysis disasters is high, and patients are condemned to a grim round of treatments that are not only painful and debilitating but often medically harmful. “The survival rate in the United States, where around 22 percent of patients die every year, is the lowest in the industrialized world,” says Leonard Stern. “The mortality in Japan is only 5 to 6 percent per year, and in Western Europe it’s in the range of 9 to 12 percent per year. So what is the difference? Well, for a start, most dialyzing in the United States is done for profit, and the for-profit survival is always less than the not-for-profit.”
After watching for decades the rise of for-profit dialysis in America and the steady degradation of care, many experienced nephrologists like John Agar and Leonard Stern have seen enough. “For many years now, I’ve been telling my American colleagues, ‘You have to stop killing your patients,’ ” Agar says.
__________________________________
Excerpted from How to Make a Killing: Blood, Death and Dollars in American Medicine by Tom Mueller. Copyright © 2023. Available from W.W. Norton & Company.